POST BURN CONTRACTURE HAND
Post burn scar contracture of the hand is one of the common deformities following a burn injury. The acute phase of a burn injury involving the hand should be managed by proper splintage in the functional position and early physiotherapy. Surgical intervention must be done wherever indicated. Post burn deformities of the hand can be reduced by proper care during the acute phase. The outcome of treatment should help in improving the functions of hand and be aesthetically acceptable.
CASE REPORT
Mr. Vijay aged 24 yrs, a case of post electric burn contracture, involving the right middle and ring finger, was seen at the outpatient clinic, with c/o inability to extend the mid and ring finger of the right hand. Clinical examination revealed a post –burn scar and flexor contracture involving the right middle and ring finger and Capsular Contracture involving PIP joint of middle finger.
TREATMENT
Stage I - Post Burn Contracture release and groin flap cover to the right mid and Ring finger Capsulotomy of PIP it of mid finger.
Stage II - Groin flap Division and Inset after 2 weeks.
Stage III- Staged Flexor Tendon reconstruction Insertion of silastic Rod and pulley reconstruction to right mid finger. Stage IV-Removal of silastic Rod and flexor Tendon reconstruction with Palmaris Long us Tendon graft.
Stage V - Hand was immobilised in a Splint for 4 weeks after Tendon reconstruction commenced on a Physiotherapy regime after removal of splint.
Follow up after 3 months showed a good range of flexion and extension of middle and ring fingers of the righ hand.
Reconstructive Surgery

Contracture right Mid & Ring finger
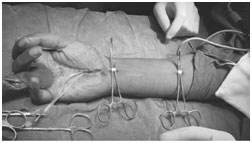
Flexor Tendon Reconstruction

Flexor Tendon Reconstruction

Groin FLAP INSITU
SUMMARY
Functions of Hand which include the ability to grasp objects and pinch must be restored for a good outcome. Burn deformities occur due to skin loss and due to secondary changes in the joints and musculotendinous units. Assessment of the deformity is very crucial for planning the treatment. The final outcome should enable the thumb to oppose the tips of finger, fingers to be straight and MCP joints to achieve flexion. Reconstruction involves skin graft or skin flaps depending on the depth of tissue loss and exposure of tendon or joints.
For a Successful outcome, proper post operative care (splintage, krischner wire fixation) and the assistance of a good physiotherapist is required.